 The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.
The information on this site is from one of the most famous books about the New Medicine (GNM / 5BN): "The Psychic Roots of Diseases" by Björn Eybl. Since September 2025, it is available in the form of an app with many additional features.It was written in german and was translated into more than 10 languages already. German is not freely available, as the rights are held by a publisher, but all these translations are available as ebooks / PDFs for free, as a gift of Björn for you, for the New Earth, for a new time.
In cooperation with Björn, it is splitted on "Disease is Different" into the sections by organ systems and combined with the real cases of our international testimonial / report archive of the related organ system.
EXTERNAL FEMALE SEX ORGANS (VULVA)
The vulva is made up of the larger, outer lips (labia majora) and the smaller inner lips (labia minor), the clitoris, the pudendal cleft, the entrance to the vagina (vaginal vestibule) and the vagina itself. The outer lips belong to the epidermis and have dermis under the epithelium. The inner lips belong to the urogenital tract and, like the vagina, they have endodermal submucosa under the ectodermal mucosa.
The vagina is a muscle tract that is about 10 cm (4 in) long, and it joins the outer genitalia with the uterus.
Located in the vaginal vestibule are endodermal glands, called Bartholin‘s glands, which secrete a lubricant upon sexual arousal.
Superficial Mucosa, Epidermis
in the Genital Area
Separation conflict
Dermis, Epidermis and Outer Lips
Attitude/perception and/or a
defilement conflict
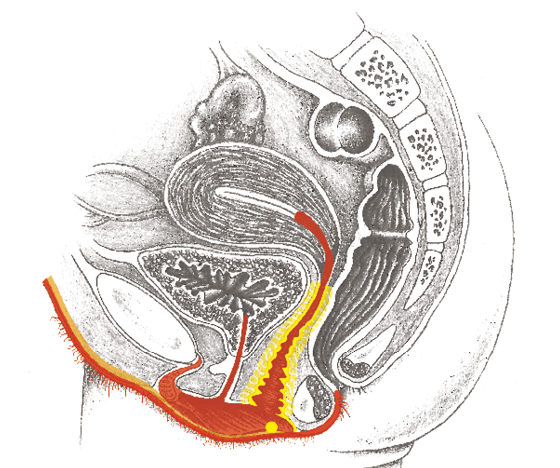
Vaginal Submucosa (yellow group)
Wanting/not wanting the penis
Vaginal Musculature
Not being able to prevent penetration or not being able to hold on to the penis
Bartholin‘s Glands
Conflict of vaginal
lubrication/dryness
Vaginal cramps (vaginismus)
The vagina is a muscular tube of smooth (involuntary) muscle.
As in the intestine, the muscles run longitudinally or ring-like.
A vaginal cramp causes the ring-like muscles to tighten, so that entry is made very difficult if not impossible.
| Conflict | Chunk conflict (see: p.15, 16: being unable to prevent penetration or not being able to hold onto the penis. |
|---|---|
| Example | ➜ A woman is forced to have sex against her will or she wants to, but cannot. |
| Conflict-active | Conflict–active A tensing-up of the involuntary vaginal ring musculature, vaginal muscle strengthening, narrowing of the vagina, vaginal tension. |
| Bio. function | With increased tension of the vaginal ring muscles, a undesired penetration can be better prevented, or the penis (desired) can be better retained. |
| Repair phase | Easing of the tension. |
| Repair crisis | Vaginal cramps (tonic-clonic seizures). |
| Note | If the subject of sexuality has a negative connotation (parental conditioning), small events or complications (e.g., the first sexual contact) are probably enough to set this SBS in motion. |
| Therapy | Determine the conflict, trigger(s) and conditioning and resolve them in real life, so the tension eases. See also: remedies for the genitalia p. 310. |

Inflammation of the outer genital area (vulvitis), vaginal inflammation (colpitis), vaginal epithelial cancer (squamous cell cancer, papillomas), genital warts (condyloma, condylomata acuminata, HPV-induced cell proliferation)
| Conflict | Separation conflict, wanting or not wanting to be touched on the vulva or vagina, wanting or not wanting to have sexual intercourse. |
|---|---|
| Examples | ➜ A woman would rather just cuddle. Her husband wants sex = conflict of not wanting sexual intercourse. Following two bitter disappointments, a woman longs for a genuine partner, not just somebody who wants sex = separation conflict of not having the desired skin contact > degradation of epithelial tissue in the active-phase. When she finds a real partner, she suffers from itching in the outer genital area for one year = repair phase, restoration of the lost substance; false diagnosis by conventional doctors: “vaginal fungus.“ (Archive B. Eybl) A woman was raped by a man when she was a young girl. Since then, she has a sexual trigger with inflammation and itching of the external genitals in the repair phase after sexual intercourse. (Archive B. Eybl) Following two bitter disappointments, a woman longs for a genuine partner, not just somebody who wants sex = separation conflict of not having the desired skin contact > degradation of epithelial tissue in the active-phase. When she finds a real partner, she suffers from itching in the outer genital area for one year = repair phase, restoration of the lost substance; false diagnosis by conventional doctors: “vaginal fungus.“ (Archive B. Eybl) A woman was raped by a man when she was a young girl. Since then, she has a sexual trigger with inflammation and itching of the external genitals in the repair phase after sexual intercourse. (Archive B. Eybl) |
| Conflict-active | Conflict–active Mostly unnoticed degradation of squamous cells of the labia, vagina or clitoris (= ulcer-cancer). No pain, possibly numbness. |
| Bio. function | The numbness (reduced sensitivity) allows the lacking or unwanted skin contact to be forgotten temporarily. |
| Repair phase | Restoration of the epithelium – inflammation of the labia, vagina, clitoris (squamous cell cancer), itching, pain, reddening, swelling; in CM, usually mistakenly diagnosed as “fungal infection“ or “herpes vulvitis,“ genital warts in persistent repair: excessive local repair of the epithelium. |
| Questions | Inflammation since when? (The conflict must have been resolved immediately before – i.e., one enjoyed the sexual activity or being left alone). First inflammation? (No > find the original conflict. Often, the first partner is decisive). Does upbringing and/or religious dogmas play a role? (Sexual intercourse is something bad)? Did my mother also have symptoms of the sort? (Conditioning through the mother’s emotional environment)? Which (family) religious beliefs play a role? (E.g. “Sex is something dirty.” “The drive is something negative.” “Men only ever want just one thing.” “I always find the wrong one.” “One has to simply be available for the man.”) With which new attitude do I want to approach the issue of sexuality? Which old behavior pattern(s) do I want to get rid of? Which meditation would be helpful? |
| Therapy | The conflict is resolved. Support the healing process. In case of a relapse, determine the conflict and conditioning. If possible, resolve the conflict in real life. For instance, choose a sexually compatible partner, who is willing to fulfill one‘s sexual wishes. Guiding principles: “I don‘t have to if I don‘t want to.“ “I‘ll do it when I feel like it.“ “Sex is nice, but true friendship and satisfaction lie outside the physical sphere.“ Colloidal silver. CM: antibiotics and/or cortisone if necessary in intensive repair phases. Possibly surgery. See also: remedies for the genitalia p. 310. |
Chancroid (ulcus molle) in women
Same SBS as above. Both women and men can suffer from “soft chancres.” Small nodes form on the external genitals that develop into round, painful ulcers.
| Phase | Active–phase – painless cell degradation from the epithelium: local loss of substance = skin ulcer. Repair phase – restoration of the epithelium with pain. |
|---|---|
| Therapy | Determine the conflict and conditioning and, if possible, resolve them in real life if still active. Questions: see above. Possibly CM: antibiotics for intensive repair phases. See also: remedies for the genitalia p. 310. |
Sudden pain in the genital-anal region (pudendal neuralgia)
Twice as common among women as among men. Sometimes accompanied by urinary or fecal incontinence.
| Conflict | Separation conflict. Not wanting to have this contact in the genital/anal area. Forced sexual intercourse, coercion into unpleasant sexual practices. |
|---|---|
| Example | A young woman falls in love with a man and enjoys carefree sex. (Her previous relationship was disappointing in this regard). One day her boyfriend “surprises” her with anal sex. Although she had given her consent to the act beforehand, she suffered a massive separation conflict because her subconscious was “reminded” of abuse she experienced in her youth. Even though the couple doesn’t engage in this practice anymore, the experience triggered a sex “track” for her. I.e. since then, she has suffered from pudendal neuralgia, numbness in the genital-anal area and slight incontinence. As therapy, the woman worked out new ground rules with her partner: Definitely, no anal sex anymore and sex only when they’re both willing; work together to integrate/heal what happened. (Archive B. Eybl) |
| Conflict active | The pudendal nerve, a sensitive nerve that receives stimuli from the genital-anal region, limits its function > Numbness, sensory disturbances, incontinence due to reduced sphincter sensitivity. |
| Bio function | The numbness allows someone to block out the unwanted contact. |
| Healing crisis | Pudendal neuralgia: Sudden, brief severe stings/pains in the genital area, sometimes urine loss due to involuntary sphincter contractions. |
| Note | Women are affected more often because men are more likely to demand abnormal sex practices from them. Women usually desire intimate union; men fantasize about various “games” > women become an object. |
| Repair/healing | Restoration of sensitivity, end of the neuralgia. Often, a recurring conflict is present. |
| Therapy | If recurring, determine the conflict, causal conditioning and belief structures and resolve. Questions similar to questions on p. 307. Cannabis (CBD oil), colloidal silver, transdermal magnesium externally. |

Vaginal “yeast infection“ of the outer labia and externally
Beneath the squamous epithelium of the outer labia lies a layer of dermis.
| Conflict | Feeling defiled or dirtied in the genital region, violation of integrity. |
|---|---|
| Example | ➜ Coarse, unwanted practices, being called foul names, unwanted sexual intercourse. |
| Conflict-active | Conflict–active Local cell division in the dermis > thickening. |
| Bio. function | Strengthening of the dermis in order to be protected from disfigurement or harm to the integrity. |
| Repair phase | Tubercular, caseating degradation via fungi, bacteria or bacteria, swelling, reddening, itching. |
| Therapy | Should it recur, determine the conflict, trigger(s) and conditioning and resolve them. Questions: see: p. 252. Colloidal silver externally. CM: antibiotics if necessary in intensive repair phases. See also: remedies for the genitalia p. 310. |
Fungal “infection“ of the inner labia or vagina (soor vulvitis, vaginal mycosis)
A reddening and itching of the female genitals is usually diagnosed as a “fungal infection.“ Most diagnoses of this nature are usually inaccurate because these symptoms are usually related to a separation conflict. But, as in the mouth, thrush is also possible in the genital area, because underneath the superficial mucosa of the inner labia and the vagina there lies a layer of endodermal (intestinal) mucous membrane.
| Conflict | Chunk conflict (see explanations p. 15, 16): not getting or not being able to take away the penis. Simply: Wanting or not wanting sexual contact. |
|---|---|
| Examples | ➜ A woman doesn‘t want to have intercourse with her partner. ➜ A woman longs for a reunion with her beloved partner. |
| Conflict-active | Increased function, thickening of the mucosa lying under the epithelium (submucosa ). |
| Bio. function | Increased mucus production so that the penis can be better received or removed. |
| Repair phase | Tubercular caseating – white residue, intense itching, white, stinking discharge, mild fever. |
| Note | During an SBS of the intestines with intestinal fungi in the repair phase, the vaginal or labial submucosa often reacts accordingly > vaginal mycosis without separation conflict, with intestinal symptoms. |
| Therapy | The conflict is resolved, support the repair phase. Should it recur, determine the conflict, trigger(s) and conditioning and resolve them. Cream mixture: aloe vera gel + natural skin cream. Colloidal silver, Hydrogen peroxide (H2O2), DMSO externally. Possibly CM: antibiotics in intensive repair phases. See also: remedies for the genitalia p. 310. |
Inflammation of the vaginal glands (bartholinitis, Bartholin‘s cyst)
| Conflict | Chunk conflict (see explanations p. 15, 16): dry vagina, not producing enough vaginal mucus to facilitate sexual intercourse. Conflict related to sexuality. |
|---|---|
| Examples | ➜ A man is too careless and wants to penetrate his partner although she is not ready. ➜ A young woman from a strict religious upbringing sleeps with a man even though she isn’t married. She now thinks she has committed a mortal sin. |
| Conflict-active | Conflict–active Cell growth in the vaginal vestibule glands (Bartholin glands) = tumor of the vaginal glands (adeno-ca) with increased mucus production. |
| Bio. function | Increase in the mucus production so that the penis can enter more easily. |
| Repair phase | Tubercular-caseating degradation of the tumor > purulent stinking discharge, possibly mild night sweats, mild fever. Recurring-conflict: Bartholin‘s cysts. |
| Note | If the Bartholin gland ducts are swollen (syndrome) a collection of pus, up to the size of a chicken egg, can develop (= Bartholin‘s cyst or abscess), which empties spontaneously. |
| Therapy | The conflict is resolved. Support the healing. Should it recur, determine the conflict or trigger(s) and, if possible, resolve them in real life. Possibly CM: antibiotics in intensive repair phases. Possibly abscess surgery. Perform intercourse only if desired or use a lubricant. See also: remedies for the genitalia p. 310. |
Vaginal discharge (fluor genitalis), gonorrhea (colloquially called “the clap“)
A small amount of clear discharge is normal in women of childbearing age. Yellowish, whitish, brownish or bad-smelling discharge can be caused by any of the following:
- Inflammation the uterus or fallopian tubes mucosa in the repair phase (see: p.296).
- Inflammation of the Bartholin glands in the repair phase, stinking tubercular degradation of the glandular tissue (see: p.309
- Inflammation of the vaginal mucosa or submucosa in the repair phase (see pp. 307 and 309).
- Purulent bladder infection in the repair phase: tubercular, caseating degradation of endodermal bladder mucosa from the trigone > not actually a discharge, but stinking, opaque urine (see: p.288).
Therapy: according to the cause.
- Bach flowers (see p. 59): crab apple, centaury, cerato.
- Teas: melissa, yarrow, lady‘s mantle, linden blossom, sanicle, fennel.
- Colloidal silver applied externally.
- Full or half bath with hydrogen peroxide, healing earth,
- EM (see: p. 66).
- MMS (see p. 68).
- Decoction of yarrow, chamomile.
- Cream mixture: aloe vera gel and natural skin lotion.
All experience reports on the organ system „External Female Sex Organs (Vulva)“ from the International Report Archive:
| Author | Title and Overview | Keywords | ||||
|---|---|---|---|---|---|---|
 | 2024/11/28   A few years ago, I had a patient (36 RH) who had massive skin abnormalities. It was genital herpes, shingles, psoriasis, purpura, all recurring, and all in the area of the genitals and lower abdomen and inner thighs, on both sides ... | Genital herpes, shingles, psoriasis, purpura, syphilis | ||||
 | 2024/03/28 I was 18 at the time and had just had my first serious relationship. My circle of friends at the time had a hard time with this relationship and didn't recognize my boyfriend. I felt torn: ... |